
Taken from our 25 July 14 Spine-Health Powered Newsletter
The term sciatica describes the symptoms of leg pain and
possibly tingling, numbness or weakness that originates in the lower back and
travels through the buttock and down the large sciatic nerve in the back of the
leg. Sciatica (pronounced sigh‐at‐ih‐kah) is not a medical
diagnosis in and of itself ‐ it is
a symptom of an underlying medical condition.
SCIATICA NERVE PAIN
Sciatica is often characterized by one or more of the
following symptoms:
- Constant pain in only one side of the buttock or leg (rarely can occur in both legs)
- Pain that is worse when sitting
- Burning or tingling down the leg (vs. a dull ache)
- Weakness, numbness or difficulty moving the leg or foot
- A sharp pain that may make it difficult to stand up or to walk
 |
| Sciatica Nerve Inflammation Pattern |
Sciatic pain can vary from infrequent and irritating to
constant and incapacitating. Specific sciatica symptoms also vary widely in
type, location and severity, depending upon the condition causing the sciatica.
While symptoms can be very painful, it is rare that
permanent sciatic nerve damage (tissue damage) will result.
THE SCIATIC NERVE AND SCIATICA
The sciatic nerve is the largest single nerve in the body
and is composed of individual nerve roots that start by branching out from the
spine in the lower back and combine to form the "sciatic nerve." When
it is irritated, sciatica symptoms occur.
- The sciatic nerve starts in the lower back at lumbar segment 3 (L3).
- At each level of the lower spine a nerve root exits from the inside of the spine and then comes together to make up the large sciatic nerve.
- The sciatic nerve runs from the lower back, down the back of each leg
- Portions of the sciatic nerve then branch out in each leg to innervate certain parts of the leg [e.g. the buttock, thigh, calf, foot, toes]
The sciatica symptoms (e.g., leg pain, numbness, tingling,
weakness, possibly symptoms that radiate into the foot) are different depending
on where the nerve is pinched. For example, a lumbar segment 5 (L5) nerve
impingement can cause weakness in extension of the big toe and potentially in
the ankle.
THE COURSE OF SCIATICA PAIN
The incidence of sciatica increases in middle age. Rarely
occurring before age 20, the probability of experiencing sciatic pain peaks in
the 50's and then declines.
Often, a particular event or injury does not cause
sciatica, but rather it tends to develop over time. The vast majority of people
who experience sciatica get better within a few weeks or months and find painrelief with non-surgical sciatica treatment. For others, however, sciatica pain
from a pinched nerve can be severe and debilitating.
There are a few symptoms that may require immediate
medical, and possibly surgical, intervention, such as progressive neurological
symptoms (e.g. leg weakness) and/or bowel or bladder dysfunction (Cauda Equina
Syndrome).
Because sciatica is caused by an underlying medical
condition, treatment is focused on relieving the underlying causes of symptoms.
Treatment is usually self-care and/or non-surgical, but for severe or
intractable cases surgery may be an option.
MOST COMMON CAUSES OF SCIATICA
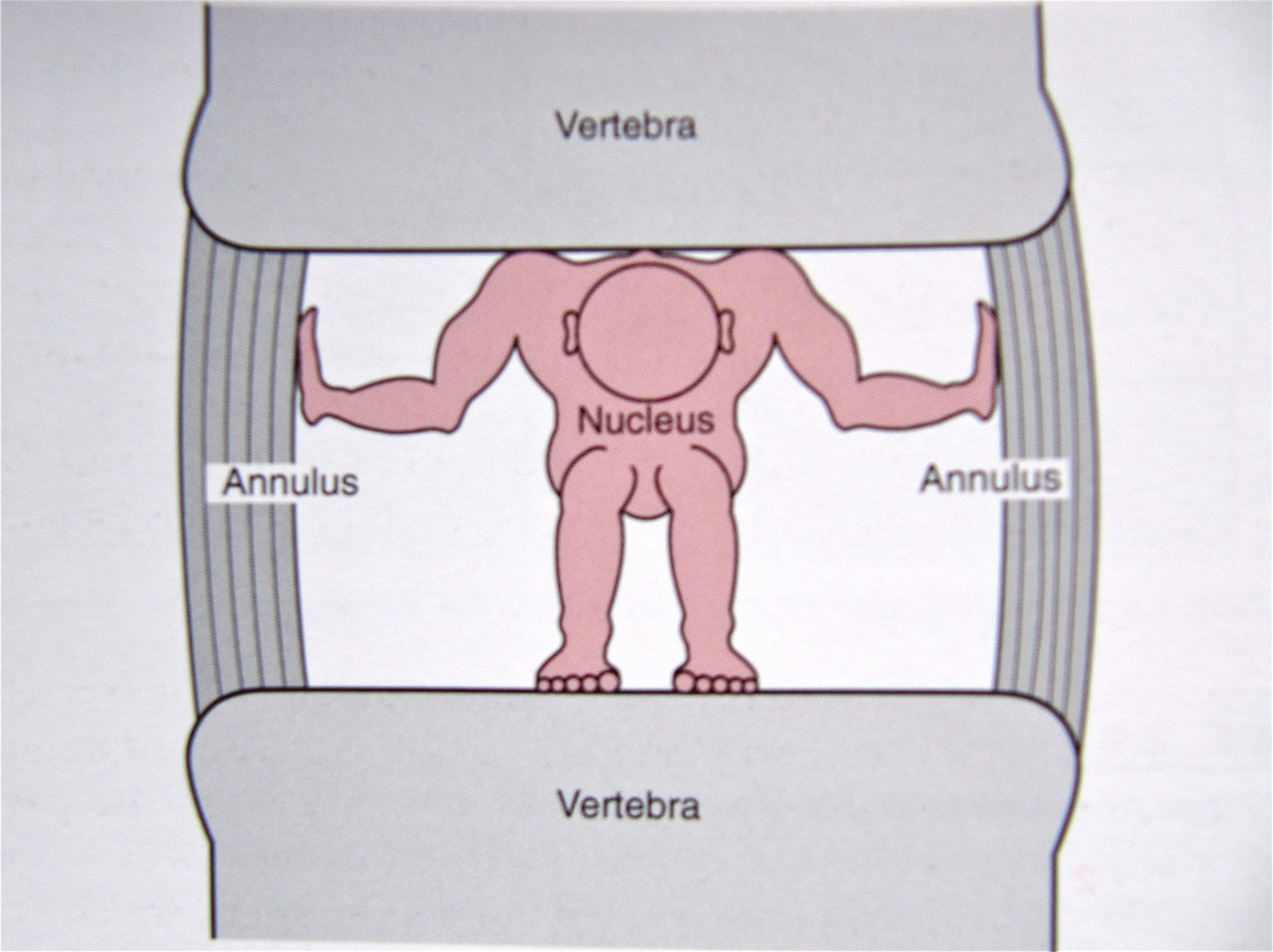
- Lumbar herniated disc (also referred to as a slipped, ruptured, bulging, or protruding disc, or a pinched nerve) occurs when the soft inner core of the disc leaks out through the outer core and irritates the nerve root. Sciatica is the most common symptom of a lumbar herniated disc.
- Degenerative disc disease is diagnosed when a weakened disc results in excessive micro-motion at that spinal level, and inflammatory proteins from inside the disc become exposed and irritate the area (including the nerve roots).
- Isthmic spondylolisthesis. This condition occurs when a small stress fracture allows one vertebral body to slip forward on another (e.g. the L5 vertebra slips over the S1 vertebra). The combination of disc space collapse, the fracture, and the vertebral body slipping forward, can cause the nerve to get pinched and cause sciatica.
- Lumbar spinal stenosis is related to natural aging in the spine and is relatively common in adults over age 60. The condition typically results from a combination of one or more of the following: enlarged facet joints, overgrowth of soft tissue, and a bulging disc placing pressure on the nerve roots, causing sciatica pain.
- Piriformis syndrome. The sciatic nerve can get irritated as it runs under the piriformis muscle in the buttock. If the piriformis muscle irritates or pinches a nerve root that comprises the sciatic nerve, it can cause sciatica- type pain.
- Sacroiliac joint dysfunction. Irritation of the sacroiliac joint - located at the bottom of the spine - can also irritate the L5 nerve, which lies on top of the sacroiliac joint, causing sciatica- type pain.
Click here to read the full article: http://www.spine-health.com/ conditions/sciatica/what-you-need-know-about-sciatica
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}