
This post was taken from our 18 July 14 Spine-Health Powered Newsletter
Each spinal disc is a unique and well-designed structure in
the spine. It is strong enough to resist terrific forces in multiple different
planes of motion, yet it is still highly mobile and permits motion in multiple
directions.
The disc has several functions,
including acting as a shock absorber between the bony vertebral bodies.
DISC ANATOMY AND FUNCTION
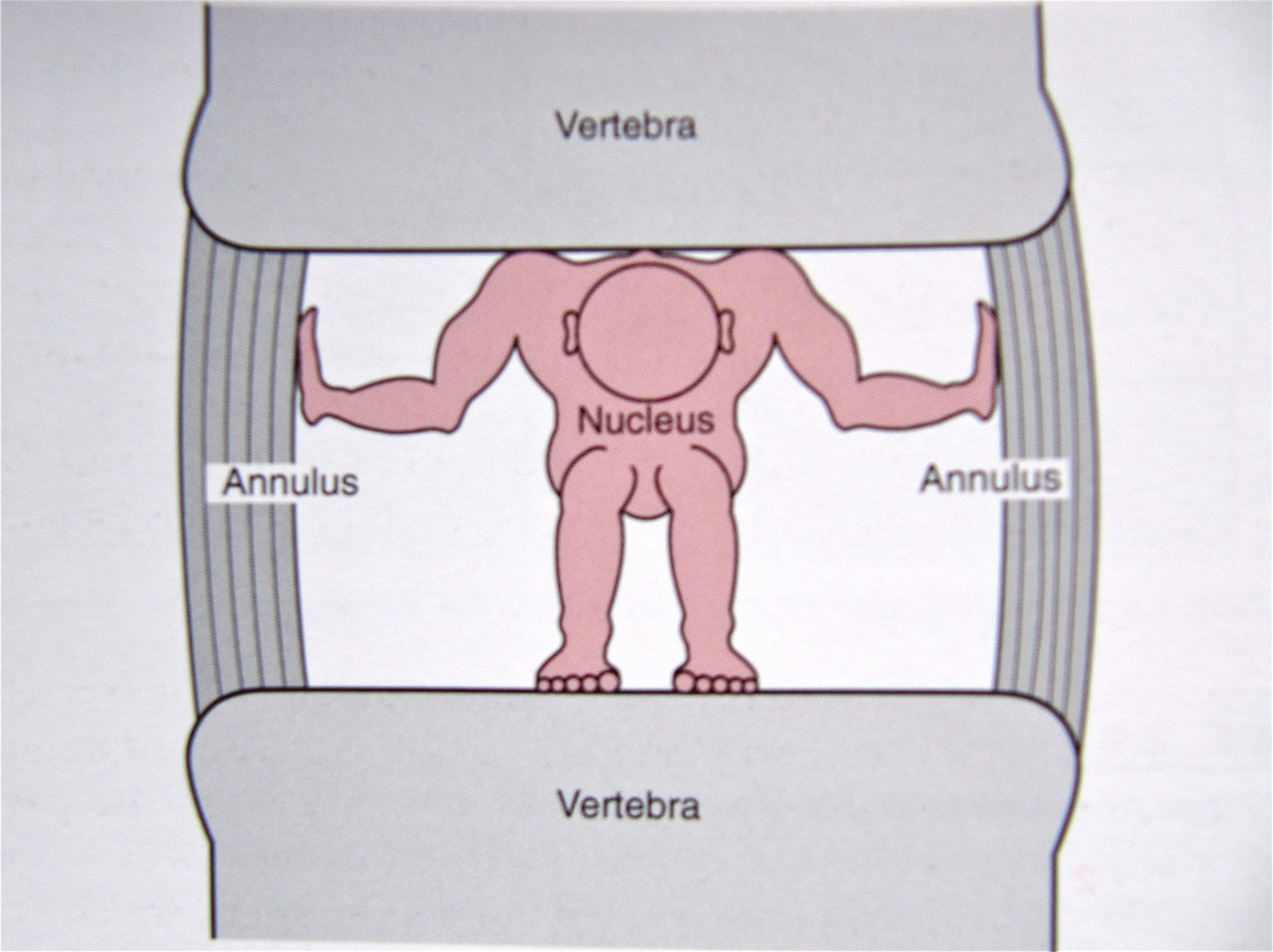
The intervertebral disc has been likened to a jelly donut.
It is comprised of a series of bands that form a tough outer layer, and soft,
jelly-like material contained within.
- Annulus Fibrosus
- the disc's firm, tough outer layer
Nerves to the disc space only penetrate into the very outer
portion of the annulus fibrosus. Even though there is little innervation to the
disc, it can become a significant source of back pain if a tear in the annulus reaches the outer portion and the nerves become
sensitized.
With continued degeneration, the nerves on the periphery of
the disc will actually grow further into the disc space and become a source of
pain.
- Nucleus Pulposus
- the jelly-like inner disc material
The inner material contained in the disc, the nucleus
pulposus, contains a great deal of inflammatory proteins. If this inner disc
material leaks out of the disc and comes in contact with a nerve root, it will
inflame the nerve root and create pain down the leg (sciatica or lumbar
radiculopathy) or down the arm (cervical radiculopathy).
When we are born, the disc is comprised of about 80% water,
which gives it its spongy quality and allows it to function as a shock
absorber. As we age, the water content decreases and the disc becomes less
capable of acting as a shock absorber
In the same manner, if any of the inflammatory proteins
within the disc space leak out to the outer annulus and touch the pain fibers in
this area, it can create a lot of low back pain or neck pain. (See
Figure 1)
The proteins within the disc space also change composition,
and most of us will develop tears into the annulus fibrosus (the outer hard
core of the disc).
Most people will have some level of disc degeneration by
their sixth decade, yet most do not have back pain (see
Figure 2).
Degenerated Disc on MRI Scan
Magnetic Resonance Imaging, called an MRI scan, has
contributed a great deal to our understanding of degenerative disc disease and
the natural degenerative process. With the advent of MRI technology, good
anatomic detail of the disc can be imaged and correlated with the individual's
pain.
Through studies with MRI scans, it was found that:
- A large number of young patients with chronic low back pain had evidence of disc degeneration on their MRI scans, and;
- Up to 30% of young healthy adults with no back pain had disc degeneration on their MRI scans.
Variability in Degenerative Disc
Disease
It is not exactly clear why some degenerated discs are
painful and some are not.
There is probably a variety of reasons that discs can
become painful.
Some theories about pain from degenerative disc disease
are:
- If a disc is injured or degenerated, it may become painful because of the resultant instability from the disc injury, which in turn can lead to an inflammatory reaction and causes low back pain.
- Some people seem to have nerve endings that penetrate more deeply into the outer annulus than others, and this is thought to make the degenerated disc more susceptible to becoming a source of pain.
While the exact
causes are not known, there is a generally agreed upon theory of how a disc
degenerates over time,....... Click here to read the full article: http://www.spine-health.com/conditions/degenerative-disc-disease/how-disc-becomes-painful
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}