Above all, life should be fun.
— Best Buddha Proverbs (@tbuddhaproverbs) October 17, 2014

Friday, October 17, 2014
“Conservative Care First” is more important today than ever in facing our nation’s healthcare challenges
Chiropractic physicians are the highest-rated healthcare practitioners for low-back pain treatments with their patient-centered, whole-person approach that provides greater interaction and communication for appropriate diagnosis and developing more cost-effective treatment planning.
October is National Chiropractic Health Month
Wednesday, September 17, 2014
Friday, June 6, 2014
The Importance of Good Posture in Reducing Back Pain
The
spine has three primary functions:
1.
It allows for movement between the different parts of the body
2.
It bears the forces applied to it
3.
It protects the spinal cord and exiting nerve roots
The
spine requires muscle force and ligament tension operating within a control
system so that it can resist buckling upon application of force (i.e. stretch, compression,
shear, torsion) and subsequently maintain equilibrium[1].[2]
This task is carried out by three distinct, yet intertwined, parts:
1. Vertebrae, spinal joints and their
capsules, intervertebral discs, and spinal ligaments make
up the Passive Musculoskeletal System.
These components produce information regarding spinal position, the load(s)
placed on each vertebra, as well as the motion (or lack thereof) of each
vertebra, and via transducers[3] provide the Neural and Feedback System this information in real time.
2. The Active Musculoskeletal System produces
the forces necessary to carry out activities of daily living while
simultaneously providing the spine its required stability. This system consists
of the muscles and tendons that surround the spine.
3. The Neural and Feedback System
determines the exact necessities for spinal stability via transducers located
in every ligament, tendon, muscle, and neural control center (spinal cord gray matter, brainstem, cerebral cortex, cerebellum, and basal ganglia) that measure the forces and motions
induced in/on the body. This sub-system then uses that information to determine
the appropriate individual muscle tensions within the active sub-system so that
it can fulfill its part of the stability mission.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
When
functioning normally these three systems work interdependently[4] with moment to moment awareness of the demands placed upon the spine (posture
as well as fixed and ambulatory[5] loads) to provide it with homeostatic
biomechanical [6] stability.
The average
person is now asking him/herself, “Why is this information important to me?”
Well this is the scientific reasoning behind why our mothers and grandmothers
were continually harping about our need to “Sit/stand up straight”. In-vitro[7]
experiments conducted at Yale and UC San Francisco found that vertebral
segments in the thoracic and lumbar
spine(s) became mechanically unstable at loads of 4.5 pound-force (20N) and
20.2 pound-force (90N) respectively.[8]
[9]
The irony of this is that the normal everyday loads placed on the spine from
body mass alone while standing are significantly larger (20-times greater) and
even more so when carrying a backpack, purse, groceries, etc. The only reason
these segments do not buckle under these forces is because of the musculature
surrounding the spine and why mindful adherence to good
ergonomics/posture is imperative in preventing back and neck injury/pain. Over
time, the stress of poor posture can change the anatomical characteristics of the spine, leading to the possibility of constricted blood vessels and nerves,
as well as problems with muscles, discs, and joints.[10]
Envision
a standard broom, better yet find a broom and with one hand grip the end of the
handle and lift the broom in the air until it’s vertical. You will find a
mechanically advantageous position once the broom is perpendicular to the floor;
at this point holding the broom aloft is almost effortless. Anatomically this
is considered “neutral position” a spinal posture in which the overall internal
stresses in the spinal column and the muscular effort to hold the posture is
minimal.[11]
Now tip the broom slightly in any direction and experience how heavy it
becomes, how much stress it now places on the wrist and arm, and how difficult
it becomes to hold aloft with one hand.[12]
This is equivalent to slouching, slumping, cradling a phone between your ear
and shoulder, looking downward too often (text-neck); habits that over time
expand the spine’s “neutral zone” and are the precedent to back and neck pain,
headaches, fatigue,
mortality
and coronary heart disease”.[13]
The
spine’s “neutral zone” is the inner region of a joint’s range of motion where
minimal resistance to motion is encountered.[2]To experience this
directly take your thumb and first finger and grip the middle knuckle of one of
the fingers on your opposite hand. Relax the gripped finger and begin to ever
so slightly wiggle the finger back and forth. The slight motion you feel within
that knuckle is the “neutral zone” which, as you've seen in this experiment, is
restricted by the ligaments alone due to your voluntary removal of the active
muscle forces that truly stabilize the joint. Poor posture and/or ergonomics
stretch the spine’s passive subsystem (spinal joint capsules,
intervertebral
discs, and spinal
ligaments) beyond its elastic limits and over time induces microtrauma which results
in expansion of the “neutral zone” altering the signals sent by the transducers
to the neural/feedback system. This places increased demands on the surrounding
musculature degrading motor
control. Consequentially inappropriate muscle
activation sequences occur during simple tasks (i.e. bending over to pick up a
piece of paper) transferring the force of these actions to the vertebral disc.
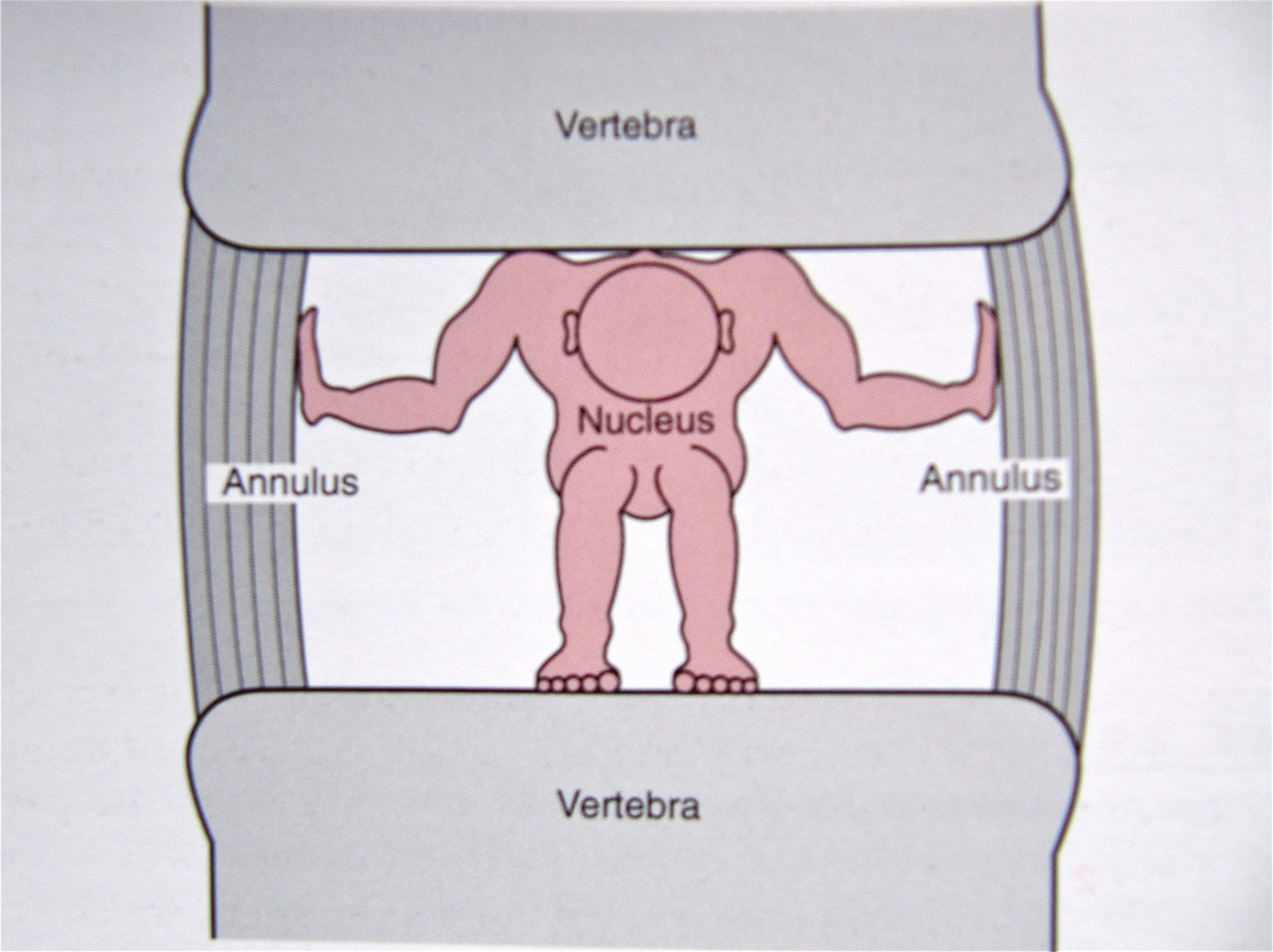
The center of the vertebral disc
contains the nucleus pulpous which
is a gelatinous cushion that protects the vertebrae from the pressures applied to the
spine. This cushion is surrounded by several layers of
fibrocartilage known as the annulus fibrosis which resemble the rings seen
inside the trunk of a tree. Unsustainable pressures applied to the disc over
time due to poor posture/ergonomics will create tearing in these rings which
results in disc bulging and eventually herniation if
one’s body mechanics/behaviors are not corrected.
{kind=link}
{kind=link}
{kind=link}
Articles and Videos to
Enhance the Importance of Good Posture/Body Mechanics
This information is not intended as a substitute for professional
medical help or advice but is to be used only as an aid in understanding back
pain.
[2]
Liebenson,
Craig. Rehabilitation of the Spine – A Practitioner’s Manual. 2nd
ed. Baltimore: Lippincott Williams& Wilkins, 2007. Print
[3]
A biological
entity that converts energy in one form to another, e.g. the rods and cones of
the eye or the hair cells of the ear
[8]
Crisco JJ. The
biomechanical stability of the human lumbar spine: experimental and theoretical
investigation [Doctoral Dissertation], New Haven, CT, Yale University, 1989
[9]
Lucas DB, Bresler
B. Stability of the ligamentous spine. Technical Report esr. 11 No. 40,
Biomechanics Laboratory, University of California at San Francisco, The
Laboratory
[10]
Schubbe, John.
"Good Posture Helps Reduce Back Pain." Spine-health: Trusted
Information for Back Pain Relief. Spine-health.com, 17 May 2004. Web. 05 June
2014. <http://www.spine-health.com/wellness/ergonomics/good-posture-helps-reduce-back-pain>.
[11]
Panjabi, Manohar
M. "The Stabilizing System of the Spine. Part II. Neutral Zone and
Instability Hypothesis." Journal of Spinal Disorders &
Techniques 5.4 (1992): 390-96. Print.
[12]
Weiniger, Steven
P. Stand Taller ~ Live Longer: An Anti-Aging Strategy: 10 Minutes a Day to Keep
Your Body Active and Pain-free. Alpharetta, GA: BodyZone, 2008. Print.
[13] S. Goya Wannamethee, PhD; A. Gerald Shaper, FRCP; Lucy Lennon, MSc; Peter H. Whincup, FRCP, PhD. "Height Loss in Older Men - Associations With Total Mortality and Incidence of Cardiovascular Disease." Arch Intern Med. 2006;166:2546-2552. Print.
[13] S. Goya Wannamethee, PhD; A. Gerald Shaper, FRCP; Lucy Lennon, MSc; Peter H. Whincup, FRCP, PhD. "Height Loss in Older Men - Associations With Total Mortality and Incidence of Cardiovascular Disease." Arch Intern Med. 2006;166:2546-2552. Print.
Tuesday, May 13, 2014
Safety of Chiropractic Care - Neck Manipulation
The efficacy of spinal manipulative therapy (SMT) has been a topic
of research for more than 20 years now and has subsequently been recognized as
such in at least four countries which has led to increased integration of
chiropractors into mainstream healthcare.[1] This
greater predominance has led to questions regarding the possibility of
complications due to SMT, especially with respect to manipulation of the cervical
spine (neck).
This was never more prevalent than after two tragic events
following chiropractic care in Canada in the 1990s which
spurred rabid media attention and an adamant stance by the neurology community
to avoid cervical manipulation as a treatment for neck pain.[2] These
events have no less been the provocative factor for the publication of several
case reports in which chiropractors have been incorrectly identified as the
practitioner responsible for injuries related to SMT.[3] This
fact is inescapable when reviewing two articles published in the Journal
of Neurology where the authors cite 46 cases involving stroke and/or
vertebral artery dissection due to “chiropractic manipulation”.
Truth be told only FOUR (4) of the cases involved chiropractors the remaining
42 cases (91%) of injury due to cervical manipulation were induced by 25
-orthopedists, 6 -physical therapists, 1 -neurologist, 2 -Primary Care
Physicians, 1 -homeopath, 2 -“health practitioners”, and the rest “remained
unreported”.[4][5][6] Admittedly
there is inherent risk, albeit minimal, associated with neck manipulation but
all forms of therapeutic intervention come with risk and some are far greater
than SMT.
Take for instance the most common “quick fix” for
musculoskeletal pain, non-steroidal anti-inflammatories [NSAIDs] (i.e. Advil,
Aleve, Motrin, Tylenol). Medical studies published during the 1990s found
that hospitalizations due to gastrointestinal complications from NSAIDs range
from 32,000 - 103,000 while NSAID related deaths average out at 9,850 ANNUALLY
in the United States alone![7][8][9] In
fact the Food and Drug Administration reports that the largest cause of drug
overdose in the United States is acetaminophen (Tylenol) which by itself is
responsible for 56,000 emergency room visits, 2,600 hospitalizations, and 458
deaths due to acute liver failure EVERY YEAR![10] The one-year
risks of experiencing complications due to prolonged NSAID use are
simply staggering: [11]
Severe gastrointestinal bleeding:
-
Adults younger than 45 = 1 in 2,100
-
Adults older than 75 = 1 in 110
Death:
-
Adults younger than 45 = 1 in 12,353
-
Adults older than 75 = 1 in 647
These non-prescription pain relievers have become an accepted form
of musculoskeletal pain relief yet their catastrophic effects have never been
as scrutinized as spinal manipulative therapy which has been scientifically
proven to be more effective in relieving neck pain and headache[12] with statistically
infinitesimal risk of serious adverse reaction.
A population based study published in Neurology in
2006 discovered that over a 16 year period (1987-2003) the incidence rate of strokes
due to arterial dissection (ICAD and VAD) affected only 0.97 - 1.72 residents per
100,000 annually within the defined community (Olmsted County, MN).[13] These
findings regarded the population in general since reliable epidemiological data was not available. A
subsequent population-based case control and case-crossover study conducted by
members of the Bone and Joint Decade 2000-2010 Task Force on Neck Pain and Its
Associated Disorders was published in SPINE in
2008 which investigated the association between chiropractic care and stroke
due to arterial dissection and compared it to primary care physician (PCP)
treatment for the same issue.[14] This
study examined ALL residents of Ontario
(109,020,875 person years), Canada’s most populous province over a nine (9)
year period (1993-2002). The researchers found only 818 cases of
stroke due to arterial dissection that met the study’s inclusion/exclusion
criteria. Overall, 4.4% (n=36) of the cases had visited a chiropractor and
51.0% (417) had only visited a PCP 30 days prior to hospital
admission for stroke related to arterial dissection. It should be noted though
that of the 36 cases noted above, only 16 cases (2.0%) were exclusively
chiropractic visits 20 (2.4%) had visited both a chiropractor and PCP with the
remaining 365 cases having consulted no one for care prior to hospitalization
due to stroke. In the end the researchers came to the following conclusions:
-
Stroke due to arterial dissection within the population is a RARE EVENT.
- Of the
453 cases that did consult either a chiropractor or PCP prior to
hospitalization, the chief complaint upon presentation was neck pain and
headache. The researchers concluded that this similarity was due to an arterial
dissection IN PROGRESS which led these patients to seek relief of their pain.
- There
is an association between chiropractic care and arterial dissection-related
stroke within residents under the age of 45 but chiropractic care DOES NOT
exhibit any excess risk of eliciting a stroke.
- There
is an association in PCP care and arterial dissection-related stroke in ALL AGE
GROUPS.
-
Currently there exists no valid screening procedure to identify the risk of
stroke in a person presenting with neck pain and/or headache.
The substantive nature of this data is enlightening but in no way
exhausts the need for further investigation into this rare yet life altering
event. A collaborative effort between chiropractors and neurologists during
future research is needed in order to derive a feasible screening method and
eliminate the confusing and conflicting information currently being given to
patients regarding the treatment of neck pain and headache.
[1] Haldeman, Scott, Paul Carey, Murray Townsend, and Costa Papadopoulos.
"Arterial Dissections following Cervical Manipulation the Chiropractic
Experience." Canadian Medical Association Journal 165.7
(2001): 905-06. Print.
[2] Cassidy, David, Eleanor Boyle, Pierre Cote, Helen He,
Sheilah Hogg-Johnson, Frank L. Silver, and Susan J. Bondy. "Risk of
Vertebrobasilar Stroke and Chiropractic Care." Spine 33.4S
(2008): 000. Print.
[3] Terrett, AG. "Misuse of the Literature by Medical
Authors in Discussing Spinal Manipulative Therapy Injury." Journal
of Manipulative and Physiological Therapeutics 18.4 (1995): 203-10.
Print.
[4] Murphy, Donald. “Primary Spine Practitioner Training
Session III: Putting it all Together.” Community Spine Pathway Training.
Burgundy Basin Inn, Rochester. 3&4 May 2014. Lecture.
[5] Hufnagel, A., Alexander Hammers, Paul-Walter Schonle,
Klaus-Dieter Bohm, and Georg Leonhardt. "Stroke following
Chiropractic Manipulation of the Cervical Spine." Journal of
Neurology 246(8) (1999): 683-88. Print.
[6] Reuter, U., M. Hamling, I. Kavuk, K. M. Einhaupl, and
E. Schielke. "Vertebral Artery Dissections after Chiropractic Neck
Manipulation in Germany over Three Years." Journal of Neurology 253(6)
(2006): 724-30. Print.
[7] Risser, Amanda, Deirdre Donovan, John Heintzman, and Tanya Page.
"NSAID Prescribing Precautions." American Family Physician 80.12
(2009): 1371-378. American Academy of Family Physicians. American Family
Physician, 15 Dec. 2009. Web. 08 May 2014.
<http://www.aafp.org/afp/2009/1215/p1371.html#afp20091215p1371-b13>.
[8] Wolfe, Micheal, David
Lichtenstein, and Gurkirpal Singh. "Gastrointestinal Toxicity of
Nonsteroidal Anti-inflammatory Drugs." New England Journal of
Medicine 340;24 (1999): 1888-899. Print.
[9] Tarone RE, Blot WJ,
McLaughlin JK. Nonselective non-aspirin nonsteroidal anti-inflammatory drugs
and gastrointestinal bleeding. Am J Ther. 2004;11(1):17–25.
[10] June 29-30, 2009: Joint Meeting of the Drug Safety and Risk Management
Advisory Committee with the Anesthetic and Life Support Drugs Advisory
Committee and the Nonprescription Drugs Advisory Committee: Meeting
Announcement http://www.fda.gov/AdvisoryCommittees/Calendar/ucm143083.htm).
[11] Blower AL, Brooks A, Fenn GC, et al. Emergency admissions for upper
gastrointestinal disease and their relation to NSAID use. Aliment Pharm
Ther. 1997;11(2):283–291.
[12] Association, American Chiropractic. "Benefits and Risks of Neck
Pain Treatments." Acatoday.org. American Chiropractic
Association, n.d. Web. 13 May 2014. <http://www.acatoday.org/pdf/Benefits_Risks_Neck_Pain_Treatments.pdf>.
[13] Lee, VH, Brown RD Jr, Mandrekar JN, et al. Incidence and outcome of
cervical artery dissection: a population-based study. Neurology 2006;67: 1809-12
[14]Cassidy, David, Eleanor Boyle, Pierre Cote, Helen He, Sheilah
Hogg-Johnson, Frank L. Silver, and Susan J. Bondy. "Risk of
Vertebrobasilar Stroke and Chiropractic Care." Spine 33.4S
(2008): 000. Print.
Saturday, April 26, 2014
A Best Evidence Synthesis Regarding the Classification and Treatment of Neck Pain
Endorsed by the United Nations on 30 November 1999 and
officially launched on 13 January 2000 at the headquarters of the World Health
Organization in Geneva, Switzerland the Bone
and Joint Decade (BJD) is an international group of healthcare
professionals that address the substantial effect that bone and joint disorders
have on society, the healthcare system, and the individual. The goal of the BJD
is to “improve the health- related quality of life for people with
musculoskeletal disorders throughout the world by raising awareness and
promoting positive actions to combat the suffering and costs to society
associated with musculoskeletal disorders”.[1]
This patient centered organization’s motivation has been the establishment of
initiatives capable of delivering best-evidence multi-disciplinary healthcare
on a global scale.
This focus was evident with establishment of The Task Force
on Neck Pain and Its Associated Disorders in 2000. This fifty (50) member Task
Force, with members from nine (9) countries, and representing nineteen (19)
clinical and scientific disciplines/specialties was mandated with the task of publishing
a report outlining
the best current evidence regarding the risk and prognosis of neck pain, its assessment/diagnosis,
and the effectiveness and safety of invasive and non-invasive treatment methods
for neck pain. During this process they were to also identify problems with the
current literature so that future studies could be developed. The goal of this
seven year project was to empower the
public, especially individuals who suffer from neck pain or at risk of
developing it. This collaborative effort that included eight (8) universities
in four (4) countries and eleven (11) professional organizations who were
nonfinancial sponsors produced a document that has changed approaches and views
regarding neck pain as well as its
prevention, diagnosis, treatment, and management.[2]
Below is the roster of the 13-member Scientific Secretariat
who conducted the screening process of 31,878 research citations on neck pain
of which 1,203 articles were found to be relevant. 46% (552) of those were
found to be “scientifically admissible” for utilization in this synthesis of
best-evidence. Aside from this, various other members of the Task Force also
conducted four (4) original research projects during its seven year tenure, two
that examined vertebrobasilar
stroke, one that compared the outcomes of various forms of neck pain
treatment, and another that examined work absenteeism due to neck pain.
As Primary
Spine Practitioners, the
doctors at Life in Motion Chiropractic and Wellness have
found this study to be an invaluable
guideline for providing our patients with or triaging them to the most
effective treatment available for their neck pain.
Stephen W.
Greenhalgh, MA, MLIS
|
|
Gabrielle van der Velde, DC, PhD (Candidate)
“In other words, one finds much more information than any individual
clinician would be able to find, download, print, read, and digest/assimilate
should he/she be devoted to such tasks full-time for years. More specifically,
the fact that not only whiplash and nontraumatic disorders but also headaches, arm
pain, and generalized symptoms of cervical origin are included in the review is
a major strength of this work. Similarly, it’s very useful having both
nonsurgical and surgical treatments in the same publication. Moreover, grading treatments
according to the likelihood of helpfulness; reporting on prognostic factors and
using “suspected etiology” to evaluate treatments are some other examples of
the clinical orientation and practicality of this report.”
Department of
Rheumatology, Physical Medicine and Rehabilitation, Hôpital Fribourgeois –
Freiburger Spital Site de Fribourg – Freiburg, Freiburg, Germany
Service de
Rhumatologie, Médecine Physique et Rééducation, 1708, Fribourg, Switzerland
| |
[1] "Background
& Goals." THE BONE AND JOINT DECADE. World Health Organization, 13
Jan. 2000. Web. 25 Apr. 2014. <http://bjdonline.org/home/bjd-goals/>.
[2] Haldeman,
Scott, Linda Carroll, David Cassidy, Jon Schubert, and Ake Nygren. "The
Bone and Joint Decade 2000-2010 Task Force on Neck Pain and Its Associated
Disorders - Executive Summary." SPINE 33.4S (2008): S5-S7. Print.
Monday, March 17, 2014
Integrative Care for Headache Pain
Headache has been a bane of humankind for centuries and one of the most common conditions that affects the nervous system. The universally accepted premise is that pain sensitive components of the head and neck are what elicit headache.[1] It is estimated that 47% of adults will experience a headache at least once within the next year.[2]
In 1988, the International Headache Society (IHS) devised a uniform system for classifying headaches which has unequivocally aided headache research. However, the clinical application of this system is limited due to its length, intricate detail, contradictory elements, and lack of real-world observation and data.[3] In fact the World Health Organization admits that many people have their headaches inaccurately diagnosed by their health-care provider.[1] An understandable fact when primary care physicians (PCP) only receive an average of four hours of instruction on headache disorders while in medical school.[1]
This statistic in no way indicates incompetence, just inadequate training with regard to headache. A comprehensible fact given the other more fatal pathologies a PCP must learn about on an intricate level.
This does, however, lead one to theorize that the prescribed drug treatments utilized to combat headache pain may be improperly applied due to the many coinciding aspects of migraine and tension-type [4] headaches. Therefore these analgesics provide no lasting relief to the patient and out of their frustration to feel better easily leads to the development of a medication-overuse headache (MOH).[5]
An integrative approach to headache pain is the most logical way to manage this epidemic given the reasons and biologic elements that contribute to it. According to the research, especially in the case of migraine and tension-type headaches, this may be the most successful strategy to help patients overcome their headache pain.
Since the principal causative factor of headache is spine related, wouldn’t it make sense to have a physician who is specifically trained in spine related disorders be the hub of the diagnostic, management and treatment of headache pain. The doctors at Life in Motion Chiropractic and Wellness are trained Primary Spine Practitioners who can deferentially diagnosis, rule out serious pathology, and provide evidence-based management for the majority of headache patients while also integrating that care with their already established healthcare providers.
[1] Swenson, Rand and Grunnet-Nilsson, N. 2005. The Management of Headache. In: Haldeman, Scott, et al, eds. Principles and Practice of Chiropractic. New York: McGraw-Hill, pp. 999-1011
[2] "Headache Disorders." WHO. Ed. WHO Media Center. World Health Organization,
Oct. 2012. Web. 12 Mar. 2014.
Oct. 2012. Web. 12 Mar. 2014.
[3] McKenzie, Robin, Stephen May. The Cervical & Thoracic Spine – Mechanical Diagnosis & Therapy.
Raumati Beach: Spinal Publications New Zealand Ltd, 2006. Print.
Raumati Beach: Spinal Publications New Zealand Ltd, 2006. Print.
[4] Most common type of primary headache. Its mechanism may be stress-related or associated with musculoskeletal problems in the neck. [World Health Organization]
Subscribe to:
Posts (Atom)