
The
spine has three primary functions:
1.
It allows for movement between the different parts of the body
2.
It bears the forces applied to it
3.
It protects the spinal cord and exiting nerve roots
The
spine requires muscle force and ligament tension operating within a control
system so that it can resist buckling upon application of force (i.e. stretch, compression,
shear, torsion) and subsequently maintain equilibrium[1].[2]
This task is carried out by three distinct, yet intertwined, parts:
1. Vertebrae, spinal joints and their
capsules, intervertebral discs, and spinal ligaments make
up the Passive Musculoskeletal System.
These components produce information regarding spinal position, the load(s)
placed on each vertebra, as well as the motion (or lack thereof) of each
vertebra, and via transducers[3] provide the Neural and Feedback System this information in real time.
2. The Active Musculoskeletal System produces
the forces necessary to carry out activities of daily living while
simultaneously providing the spine its required stability. This system consists
of the muscles and tendons that surround the spine.
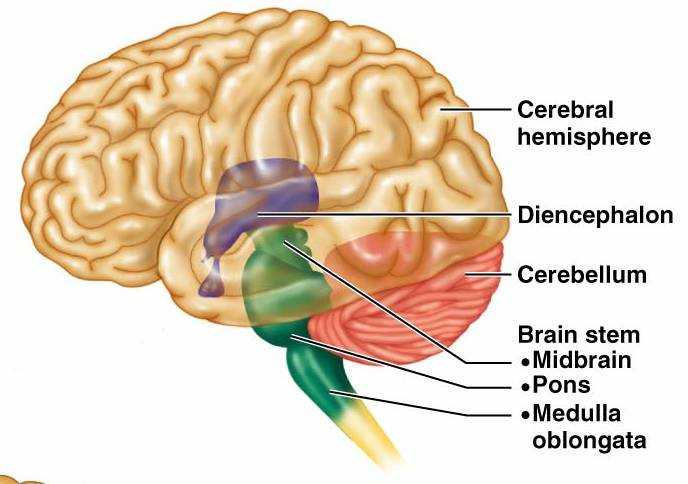
3. The Neural and Feedback System
determines the exact necessities for spinal stability via transducers located
in every ligament, tendon, muscle, and neural control center (spinal cord gray matter, brainstem, cerebral cortex, cerebellum, and basal ganglia) that measure the forces and motions
induced in/on the body. This sub-system then uses that information to determine
the appropriate individual muscle tensions within the active sub-system so that
it can fulfill its part of the stability mission.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
When
functioning normally these three systems work interdependently[4] with moment to moment awareness of the demands placed upon the spine (posture
as well as fixed and ambulatory[5] loads) to provide it with homeostatic
biomechanical [6] stability.
The average
person is now asking him/herself, “Why is this information important to me?”
Well this is the scientific reasoning behind why our mothers and grandmothers
were continually harping about our need to “Sit/stand up straight”. In-vitro[7]
experiments conducted at Yale and UC San Francisco found that vertebral
segments in the thoracic and lumbar
spine(s) became mechanically unstable at loads of 4.5 pound-force (20N) and
20.2 pound-force (90N) respectively.[8]
[9]
The irony of this is that the normal everyday loads placed on the spine from
body mass alone while standing are significantly larger (20-times greater) and
even more so when carrying a backpack, purse, groceries, etc. The only reason
these segments do not buckle under these forces is because of the musculature
surrounding the spine and why mindful adherence to good
ergonomics/posture is imperative in preventing back and neck injury/pain. Over
time, the stress of poor posture can change the anatomical characteristics of the spine, leading to the possibility of constricted blood vessels and nerves,
as well as problems with muscles, discs, and joints.[10]
Envision
a standard broom, better yet find a broom and with one hand grip the end of the
handle and lift the broom in the air until it’s vertical. You will find a
mechanically advantageous position once the broom is perpendicular to the floor;
at this point holding the broom aloft is almost effortless. Anatomically this
is considered “neutral position” a spinal posture in which the overall internal
stresses in the spinal column and the muscular effort to hold the posture is
minimal.[11]
Now tip the broom slightly in any direction and experience how heavy it
becomes, how much stress it now places on the wrist and arm, and how difficult
it becomes to hold aloft with one hand.[12]
This is equivalent to slouching, slumping, cradling a phone between your ear
and shoulder, looking downward too often (text-neck); habits that over time
expand the spine’s “neutral zone” and are the precedent to back and neck pain,
headaches, fatigue,
mortality
and coronary heart disease”.[13]
The
spine’s “neutral zone” is the inner region of a joint’s range of motion where
minimal resistance to motion is encountered.[2]To experience this
directly take your thumb and first finger and grip the middle knuckle of one of
the fingers on your opposite hand. Relax the gripped finger and begin to ever
so slightly wiggle the finger back and forth. The slight motion you feel within
that knuckle is the “neutral zone” which, as you've seen in this experiment, is
restricted by the ligaments alone due to your voluntary removal of the active
muscle forces that truly stabilize the joint. Poor posture and/or ergonomics
stretch the spine’s passive subsystem (spinal joint capsules,
intervertebral
discs, and spinal
ligaments) beyond its elastic limits and over time induces microtrauma which results
in expansion of the “neutral zone” altering the signals sent by the transducers
to the neural/feedback system. This places increased demands on the surrounding
musculature degrading motor
control. Consequentially inappropriate muscle
activation sequences occur during simple tasks (i.e. bending over to pick up a
piece of paper) transferring the force of these actions to the vertebral disc.
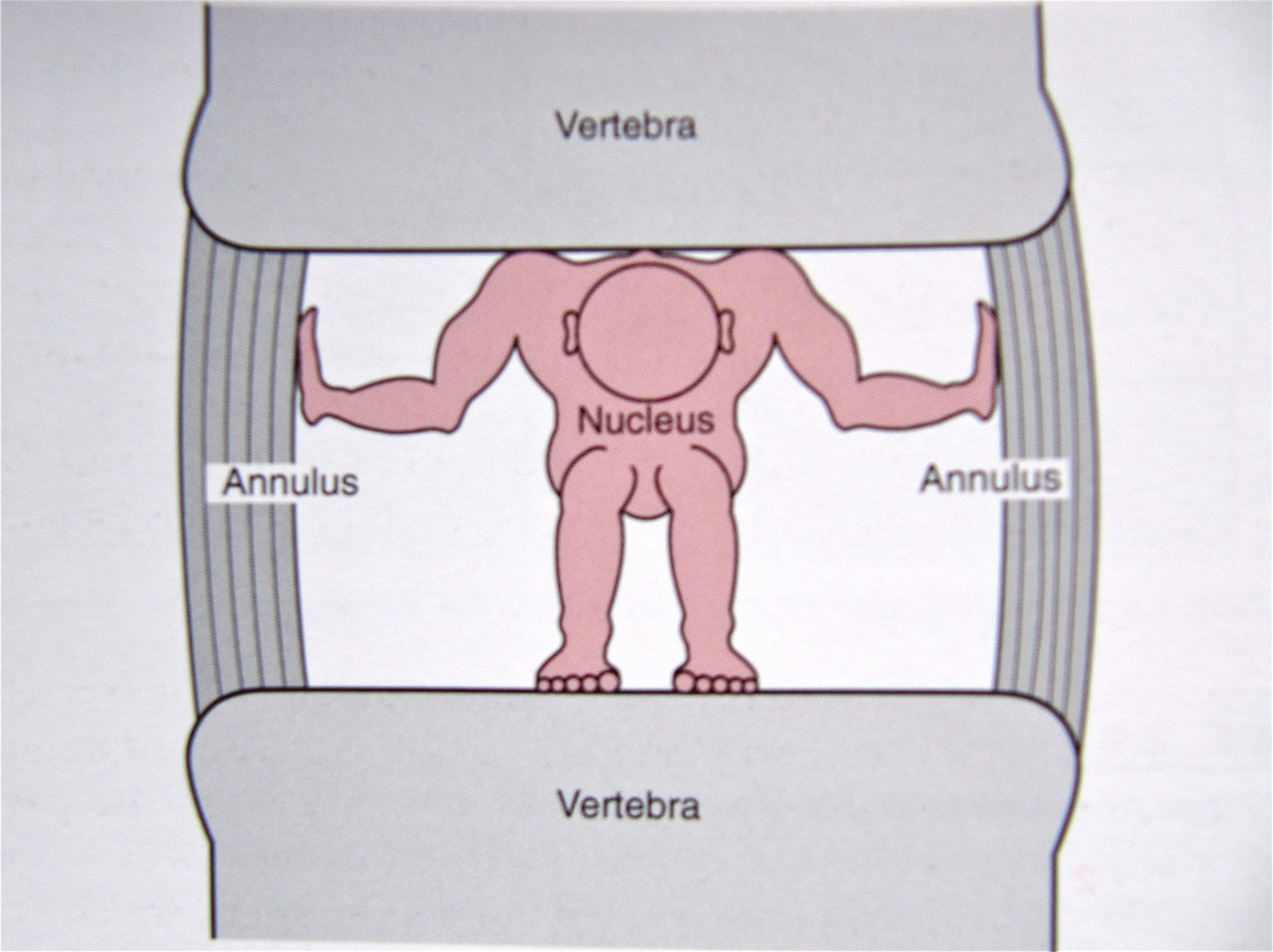
The center of the vertebral disc
contains the nucleus pulpous which
is a gelatinous cushion that protects the vertebrae from the pressures applied to the
spine. This cushion is surrounded by several layers of
fibrocartilage known as the annulus fibrosis which resemble the rings seen
inside the trunk of a tree. Unsustainable pressures applied to the disc over
time due to poor posture/ergonomics will create tearing in these rings which
results in disc bulging and eventually herniation if
one’s body mechanics/behaviors are not corrected.
{kind=link}
{kind=link}
{kind=link}
Articles and Videos to
Enhance the Importance of Good Posture/Body Mechanics
This information is not intended as a substitute for professional
medical help or advice but is to be used only as an aid in understanding back
pain.
[2]
Liebenson,
Craig. Rehabilitation of the Spine – A Practitioner’s Manual. 2nd
ed. Baltimore: Lippincott Williams& Wilkins, 2007. Print
[3]
A biological
entity that converts energy in one form to another, e.g. the rods and cones of
the eye or the hair cells of the ear
[8]
Crisco JJ. The
biomechanical stability of the human lumbar spine: experimental and theoretical
investigation [Doctoral Dissertation], New Haven, CT, Yale University, 1989
[9]
Lucas DB, Bresler
B. Stability of the ligamentous spine. Technical Report esr. 11 No. 40,
Biomechanics Laboratory, University of California at San Francisco, The
Laboratory
[10]
Schubbe, John.
"Good Posture Helps Reduce Back Pain." Spine-health: Trusted
Information for Back Pain Relief. Spine-health.com, 17 May 2004. Web. 05 June
2014. <http://www.spine-health.com/wellness/ergonomics/good-posture-helps-reduce-back-pain>.
[11]
Panjabi, Manohar
M. "The Stabilizing System of the Spine. Part II. Neutral Zone and
Instability Hypothesis." Journal of Spinal Disorders &
Techniques 5.4 (1992): 390-96. Print.
[12]
Weiniger, Steven
P. Stand Taller ~ Live Longer: An Anti-Aging Strategy: 10 Minutes a Day to Keep
Your Body Active and Pain-free. Alpharetta, GA: BodyZone, 2008. Print.
[13] S. Goya Wannamethee, PhD; A. Gerald Shaper, FRCP; Lucy Lennon, MSc; Peter H. Whincup, FRCP, PhD. "Height Loss in Older Men - Associations With Total Mortality and Incidence of Cardiovascular Disease." Arch Intern Med. 2006;166:2546-2552. Print.
[13] S. Goya Wannamethee, PhD; A. Gerald Shaper, FRCP; Lucy Lennon, MSc; Peter H. Whincup, FRCP, PhD. "Height Loss in Older Men - Associations With Total Mortality and Incidence of Cardiovascular Disease." Arch Intern Med. 2006;166:2546-2552. Print.